Dental and medical billing share a goal: get the provider paid for services rendered. But almost everything about how they get there is different. Code sets, claim forms, payer types, reimbursement rules, even the way denials are appealed. Anyone running a dental practice or moving between dental and medical billing roles needs to understand where the lines are drawn.
Different code sets
Medical billing uses CPT (Current Procedural Terminology) for services and ICD-10 for diagnoses. The American Medical Association maintains CPT and the National Center for Health Statistics maintains ICD-10. Together they describe what was done and why.
Dental billing uses CDT (Current Dental Terminology), maintained by the American Dental Association. CDT codes are dental-specific and capture the procedure, the tooth, the surface, and sometimes the quadrant. ICD-10 is occasionally used in dental claims for medical necessity (typically only for cross-billing to medical), but most dental claims rely on CDT alone.
Examples of how the same idea is coded differently:
- A routine office visit: CPT 99213 (medical) versus D0120 (dental periodic exam).
- A simple radiograph: CPT 70220 (medical x-ray) versus D0220 (dental periapical).
- A surgical procedure: CPT 41899 (oral and maxillofacial unlisted, medical) versus D7140 (dental extraction, dental).
Different claim forms
Medical claims go on the CMS-1500 (for professional services) or UB-04 (for facility services). These are standardized HIPAA forms accepted by every medical payer in the U.S.
Dental claims go on the ADA Dental Claim Form (the 2019 or 2024 version, depending on payer). Same idea, different layout, different required fields. The ADA form has tooth diagrams, surface notation, and quadrant identifiers that don’t appear on a CMS-1500.
Different payer mix
Medical billers work with hundreds of payers including Medicare, Medicaid, commercial insurers (Aetna, Cigna, BCBS, UnitedHealthcare), and TriCare. Reimbursement rates are heavily regulated and the rules are publicly published.
Dental billers work with a smaller, more concentrated set of payers: Delta Dental (the largest), MetLife, Cigna Dental, Aetna Dental, Guardian, and a long tail of regional plans. Medicare doesn’t cover most adult dental services. Medicaid dental coverage varies wildly by state. Reimbursement rates are negotiated per network and are often confidential.
Different reimbursement structures
Medical reimbursement is built around fee schedules, RVUs (Relative Value Units), and increasingly value-based contracts where reimbursement depends on outcomes. Bundling rules and modifiers (like 25 and 59) are central to medical billing.
Dental reimbursement is simpler in some ways and harder in others. Most dental plans have:
- A flat annual maximum (typically $1,500 to $2,500).
- A deductible (usually $50 individual, $150 family).
- Coinsurance tiers (100 percent preventive, 80 percent basic, 50 percent major).
- Frequency limitations on common procedures.
- A missing-tooth clause (won’t pay for a prosthetic on a tooth lost before the policy started).
The annual maximum is the single biggest difference. Once a patient hits $1,500 in dental benefits, the plan stops paying. There’s no equivalent ceiling on most medical plans.
Predeterminations versus prior authorizations
Both fields use a “let’s get this approved before we do it” workflow, but the names and rules differ.
- Medical: prior authorization (sometimes called precertification) is required for high-cost procedures, imaging, and certain medications. The denial rate on requests without prior auth is high. Authorization numbers must be on the claim.
- Dental: predetermination is non-binding but strongly recommended for crowns, implants, ortho, and any procedure over $300. The predetermination tells you what the payer is likely to pay before you do the work, but it doesn’t guarantee payment if details change at delivery.
Different documentation requirements
Medical claims primarily need:
- The diagnosis (ICD-10) tied to medical necessity.
- The procedure (CPT) with appropriate modifiers.
- A clinical note that supports the level of service billed.
Dental claims primarily need:
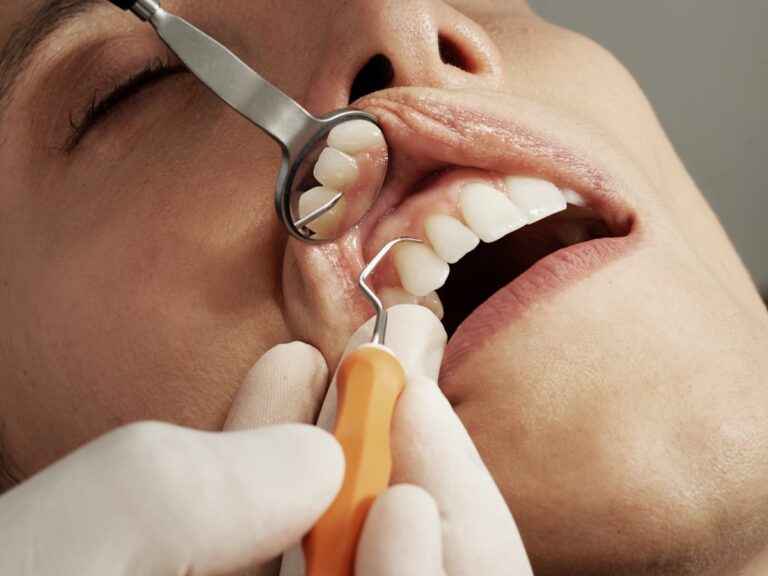
- Pre-op and post-op periapical x-rays for crowns, root canals, and extractions.
- Periodontal charting for scaling and root planing.
- A narrative explaining medical necessity for unusual procedures.
- Tooth, surface, and quadrant on every applicable line.
Different timely-filing windows
Medicare requires claims within 12 months of the date of service. Most commercial medical payers allow 90 to 180 days. Medicaid varies by state, sometimes 180 days, sometimes a year.
Dental payers are tighter. Delta Dental and most major dental insurers require claims within 90 days. Some plans require 60. Medicaid dental can be longer (up to 365 days). Late submission is the most preventable revenue loss in dental.
When dental and medical overlap
A small but important share of dental procedures should be billed to medical insurance, not dental. The most common cross-billing scenarios:
- Sleep apnea oral appliances (E0486, often covered by medical).
- Surgical extractions for impacted wisdom teeth in some plans.
- Treatment for accidents or injuries to teeth (often primarily medical).
- Biopsies of oral lesions (CPT 41100 series, medical).
- TMJ-related procedures (medical, with the right ICD-10).
Dental practices that miss these opportunities leave money on the table. Practices that abuse them risk audits.
Why this matters when hiring
A medical biller and a dental biller are two different jobs. A medical biller hired into a dental practice will struggle with CDT codes, attachment requirements, and payer-specific quirks. A dental biller asked to handle medical cross-claims needs additional CPT/ICD-10 training.
If you’re hiring in-house, hire for the specialty you’re billing. If you’re outsourcing, choose a partner whose dental team is dedicated, not generalists. The clean-claim difference between specialty-trained and generalist billers is around 8 to 12 percentage points.
The bottom line
Dental billing isn’t medical billing with a different code book. It’s a separate discipline with its own forms, payer relationships, frequency rules, and evidentiary requirements. Mixing the two without trained staff is the fastest way to grow aged A/R. Treat dental billing as the specialty it is, and the practice gets paid.
Authoritative sources
This article cites the following primary sources for billing-code and regulatory guidance. Always confirm current rules and codes with the publishing authority before applying to a specific claim.